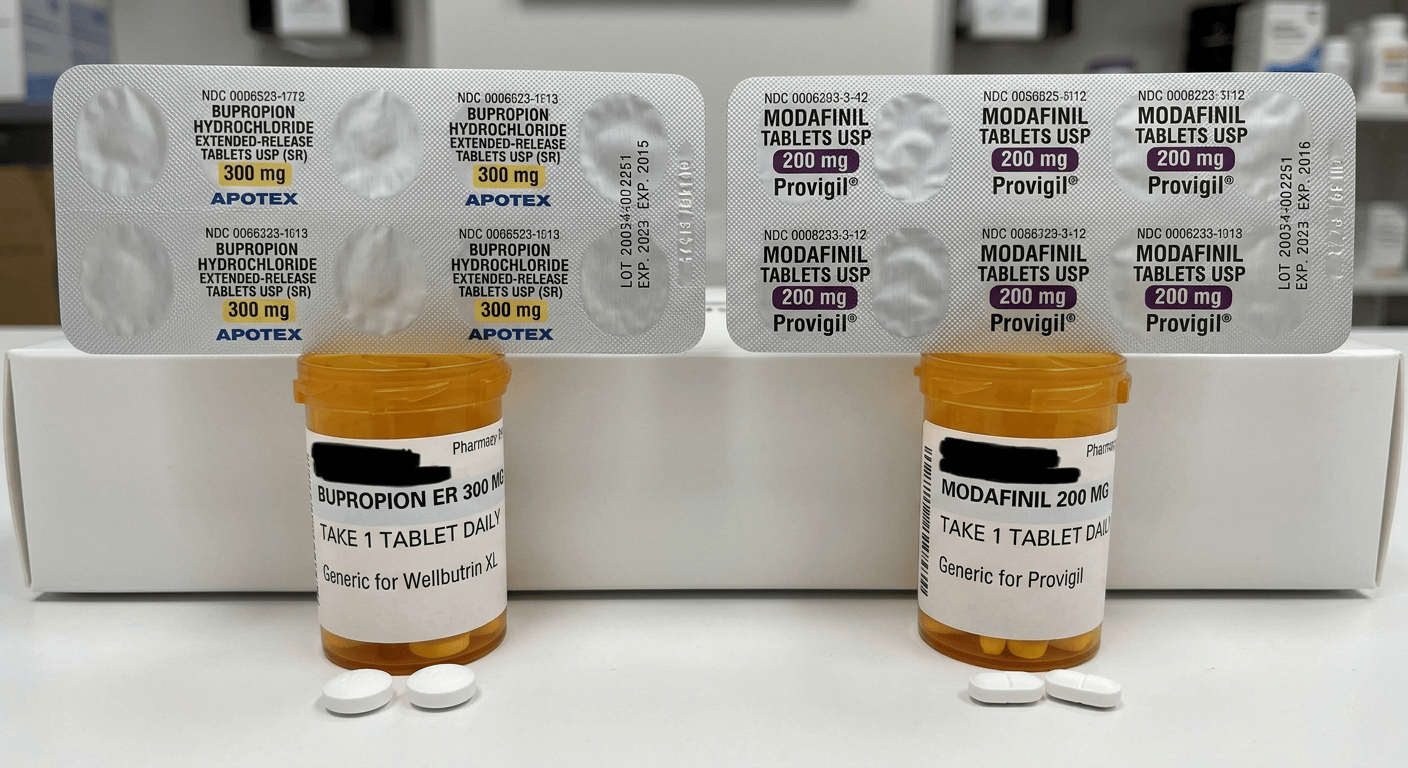
Can You Take Bupropion with Modafinil? Safety, Effects, and Interactions
The short answer
Bupropion and modafinil are not automatically contraindicated together. There is no strong evidence showing a specific, dangerous interaction unique to this pair. But that does not make the combination straightforward or low-risk.
The issue is overlap. Both drugs act on systems tied to stimulation, alertness, and catecholamines, especially dopamine and norepinephrine. That overlap raises the chance of additive effects, not in a clean, predictable way, but in a way that can amplify side effects like insomnia, anxiety, and elevated blood pressure. In the case of bupropion, seizure risk is part of that picture.

Bupropion carries a clearly documented, dose-related seizure risk, with FDA labeling estimating seizures in about 0.4 percent of patients at standard doses and sharply higher rates above that range. Modafinil does not carry the same seizure profile, but it does increase central nervous system activation and has been linked to increased need for blood pressure monitoring in some patients.
There is also a second layer of uncertainty. High-quality studies looking specifically at bupropion and modafinil as a combination are scarce. Most of what is known comes from each drug individually, not from controlled trials of the pair.
The practical takeaway is that the combination is pharmacologically plausible, but not plug-and-play. It requires a deliberate look at individual risk factors rather than a simple yes-or-no answer.
Why this combination raises eyebrows pharmacologically
Bupropion works by inhibiting the reuptake of dopamine and norepinephrine, increasing their availability in the brain. That is part of why it can improve energy, motivation, and concentration in some patients.
Modafinil is more complex, but it still affects many of the same systems. A human imaging study showed that modafinil blocks dopamine transporters and increases dopamine levels in the brain. It also influences wakefulness pathways involving orexin, histamine, and norepinephrine.
Put side by side, the overlap is clear. Both increase dopaminergic signaling and both push norepinephrine upward, even if they do it differently.
That does not mean their effects simply add together. Sometimes the combination feels synergistic, sometimes redundant, and sometimes it tips into side effects without much added benefit. The outcome depends on baseline neurochemistry, dose, timing, and individual sensitivity.
This is why the pairing draws attention. The mechanism makes intuitive sense, but the lack of strong combination-specific evidence means decisions rely on first principles rather than clear trial data.
The main risks to think about first
Three areas matter most: seizures, cardiovascular strain, and overstimulation.
Seizure risk comes almost entirely from bupropion. At standard doses up to 450 mg per day, seizures occur in roughly 0.4 percent of patients, with risk increasing sharply at higher doses. That is a measured, dose-dependent effect.
Modafinil does not carry the same established seizure signal. But it does increase central nervous system activation. There is no defined combined seizure-risk profile for the pair, which means the concern is inferential. If one drug lowers the seizure threshold and the other increases activation, the margin may narrow in people who are already vulnerable.
Cardiovascular effects are the second major piece. Bupropion can raise blood pressure, and modafinil labeling supports monitoring blood pressure and heart rate. Individually, these effects are often manageable. Together, they can stack, especially in people with borderline hypertension or sensitivity to stimulants.
Then there is overstimulation. Both drugs can disrupt sleep, increase anxiety, and produce a restless, wired feeling. When they overlap, the result is often not sharper focus but fragmented attention and difficulty winding down.
Across all three domains, the pattern is the same. There is no single interaction to point to. There is a convergence of effects that makes outcomes less predictable and more dependent on the individual.
The less obvious interaction issue, metabolism and other medications
The more complicated interaction question is not just bupropion plus modafinil. It is what happens when they are added to everything else.
Bupropion inhibits CYP2D6, which affects how many drugs are metabolized, including certain antidepressants, antipsychotics, beta blockers, and opioids. This can raise levels of those medications.
Modafinil affects a different set of pathways. It can inhibit CYP2C19 and induce CYP3A4, CYP2B6, and CYP1A2. That means it can speed up the metabolism of some drugs and slow down others.
The result is not a simple interaction pattern. It is a shifting one, depending on the rest of the medication list.
This is why the cleaner question often misses the point. Instead of asking only whether these two drugs interact, the more useful question is how they affect the broader regimen. In more complex medication setups, that secondary layer can matter as much as the primary combination.
Why someone might look into this combination in the first place
The interest in combining Bupropion and Modafinil usually starts with incomplete symptom control.
Bupropion is used for depression and sometimes off-label for ADHD. It can improve energy and motivation, but not always enough. Fatigue, brain fog, or inconsistent focus may persist.
Modafinil has been studied as an adjunct in people with depression who still struggle with excessive sleepiness or low energy. Some studies suggest modest improvements in fatigue and overall symptoms, though the evidence is small and inconsistent.
There is a similar pattern in attention-related symptoms. Bupropion shows modest benefit in adult ADHD, while modafinil has mixed evidence and remains off-label. Neither is first-line, but both are considered in specific situations.
Put together, the logic is practical rather than guideline-driven. The combination is not standard treatment. It is an attempt to address overlapping symptoms that one medication alone has not resolved.
What the evidence does and does not say
There is no strong Tier 1–3 evidence directly studying the routine use of bupropion and modafinil together. No large randomized trials. No clear clinical guidelines built around this pairing.
What exists is indirect.
One layer comes from regulatory data and pharmacology, showing how each drug behaves individually. Another comes from adjunctive studies of modafinil in depression, which suggest possible benefits for fatigue in some patients. A third comes from off-label use contexts like ADHD.
What is missing is direct combination data. Without that, there is no reliable way to quantify how often the pairing helps, how often it causes problems, or who benefits most.
That limitation matters. It keeps the article from making claims that the literature does not support. The answer rests on mechanism and individual risk, not established protocols.
Who should be especially cautious
Some people can approach this as a careful medication question. Others start closer to the edge.
Anyone with a higher baseline seizure risk should be cautious. That includes people with seizure disorders, eating disorders, heavy alcohol use, or medications that lower seizure threshold. Bupropion is the main driver, but adding another activating drug does not improve that margin.
People with uncontrolled high blood pressure or cardiovascular disease also deserve caution. Both drugs can push blood pressure upward.
Anxiety and insomnia are often the limiting factors in practice. Someone already struggling with sleep or overstimulation may find the combination destabilizing rather than helpful.
There is also the question of mood stability. In people with a history of activation or mood swings with stimulating medications, adding a second activating agent deserves extra scrutiny.
Finally, polypharmacy matters. The more complex the medication list, the more relevant CYP-related interactions become. In those cases, the combination is not just about two drugs. It is about how the entire regimen shifts.
Bottom line
Taken together, Bupropion and Modafinil are not inherently incompatible. But they are not a simple pairing either.
They push in similar physiological directions. That overlap explains both the appeal and the risk. In some cases, it may help address persistent fatigue or attention problems. In others, it amplifies side effects without adding much benefit.
The most reliable way to approach the combination is through what is known:
- bupropion’s seizure risk and CYP2D6 inhibition,
- modafinil’s activating effects and CYP profile,
- and the lack of strong evidence specifically studying the pair.
That last point anchors the decision. The combination exists in a space where individual drug data is clear, but combination data is thin.
A useful discussion focuses less on whether the pairing is allowed and more on whether the individual has the margin for it. Seizure risk, blood pressure, sleep, anxiety, and the rest of the medication list matter more than the theoretical compatibility of the drugs.
That is where the real answer sits.
Sources
A. Peer-Reviewed Studies
Volkow, N. D., Fowler, J. S., Logan, J., Alexoff, D., Zhu, W., Telang, F., Wang, G. J., Jayne, M., Hooker, J. M., Wong, C., Hubbard, B., Carter, P., Warner, D., King, P., Shea, C., Xu, Y., Muench, L., & Apelskog-Torres, K. (2009). Effects of modafinil on dopamine and dopamine transporters in the male human brain: Clinical implications. JAMA, 301(11), 1148–1154. https://jamanetwork.com/journals/jama/fullarticle/183580
Goss, A. J., Kaser, M., Costafreda, S. G., Sahakian, B. J., & Fu, C. H. Y. (2013). Modafinil augmentation therapy in unipolar and bipolar depression: A systematic review and meta-analysis. Journal of Clinical Psychiatry, 74(11), 1101–1107. https://pubmed.ncbi.nlm.nih.gov/24330897/
Fava, M., Thase, M. E., DeBattista, C., Doghramji, K., Arora, S., Hughes, R. J., & Modafinil Study Group. (2005). Modafinil augmentation of selective serotonin reuptake inhibitor therapy in MDD partial responders. Biological Psychiatry, 57(4), 464–470. https://pubmed.ncbi.nlm.nih.gov/17729016/
Schwartz, T. L., Siddiqui, U. A., & Raza, S. (2005). Modafinil as adjunctive therapy in depression. Annals of Clinical Psychiatry, 17(3), 153–159. https://pubmed.ncbi.nlm.nih.gov/15367049/
Verbeeck, W., Tuinier, S., & Bekkering, G. E. (2017). Bupropion for attention deficit hyperactivity disorder (ADHD) in adults. Cochrane Database of Systematic Reviews, 2017(10), CD009504. https://pubmed.ncbi.nlm.nih.gov/28965364/
Wilens, T. E., Spencer, T. J., Biederman, J., Prince, J., Monuteaux, M. C., & Soriano, J. (2005). A controlled clinical trial of bupropion for attention deficit hyperactivity disorder in adults. American Journal of Psychiatry, 162(6), 1242–1244. https://pubmed.ncbi.nlm.nih.gov/15820237/
Turner, D. C., Clark, L., Pomarol-Clotet, E., McKenna, P. J., & Robbins, T. W. (2004). Modafinil improves cognition and response inhibition in adult attention-deficit/hyperactivity disorder. Biological Psychiatry, 55(10), 1031–1040. https://pubmed.ncbi.nlm.nih.gov/15023577/
B. Institutional & Other Sources
U.S. Food and Drug Administration. (2024). Wellbutrin (bupropion) prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/018644s061lbl.pdf
U.S. Food and Drug Administration. (2024). Wellbutrin XL (bupropion) prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/021515s046lbl.pdf
U.S. Food and Drug Administration. (2015). Provigil (modafinil) prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020717s037s038lbl.pdf
U.S. Food and Drug Administration. (2010). Provigil (modafinil) clinical pharmacology. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/020717s030s034s036lbl.pdf
Preskorn, S. H., Shah, R., Neff, M., Golbeck, A., & Choi, J. (2007). Comparison of the tolerability of bupropion and SSRIs: Pharmacokinetic considerations. Journal of Psychiatric Practice, 13(5), 296–304. https://pubmed.ncbi.nlm.nih.gov/15876900/
Robertson, P., Hellriegel, E. T., Arora, S., & Nelson, M. (2003). Effect of modafinil on the pharmacokinetics of other drugs. Clinical Pharmacokinetics, 42(2), 123–137. https://pubmed.ncbi.nlm.nih.gov/12537513/